What is a distal femoral osteotomy?
A distal femoral osteotomy (knock knee surgery) is a procedure whereby a surgical fracture is created at the end of the femur and the shape of the bone is changed. In general, these are performed for patients with knock knees, which we call valgus alignment, and the goal of the surgery is to realign them such that the weightbearing axis is changed to pass either through the center of the knee or just barely into the inside compartment of the knee.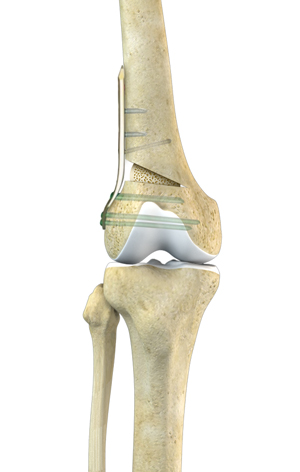
What are the Different Indications of Distal Femoral Osteotomies?
There are usually 3 main indications for distal femoral osteotomies. The first one is in patients who may have developed arthritis either from a previous lateral meniscectomy or genetic causes and who are found to have fairly normal cartilage in the rest of their knee, but have arthritis on the outside of their knee. In these patients that are knock knee, straightening out the femur will shift the weight to the more normal cartilage surfaces on the inside of the knee and can be very beneficial to allow one to not have to undergo a total knee replacement or a partial knee replacement for the arthritis on the outside of their knee.The next most common indication for a distal femoral osteotomy is when a patient is knock knee and needs a lateral meniscal transplant and/or a cartilage resurfacing procedure of the outside (lateral) compartment of their knee. The success rates for lateral meniscal transplants and cartilage resurfacing procedures are much less if the valgus alignment is not corrected with the surgical procedure (or before it). The third most common reason for a distal femoral osteotomy is in patients who have a chronic MCL tear who are in valgus alignment. It is felt that if the valgus alignment is not corrected with a reconstruction of a chronic MCL tear, that there is a much higher risk the MCL tear will stretch out.
What is the Most Common Type of Distal Femoral Osteotomy?
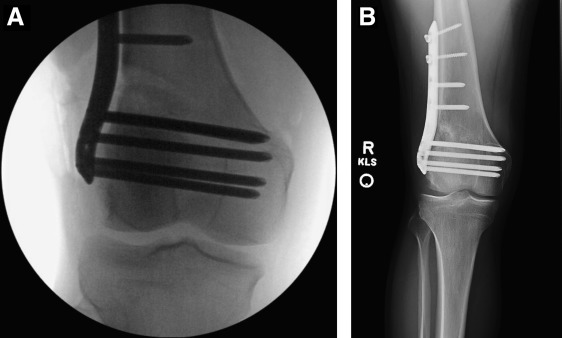
The most common type of distal femoral osteotomy is one that involves an incision on the outside of the knee. The femur is cut with surgical instruments to about 1 cm away from the medial edge of the femur, commonly at a 45-degree angle and angling towards the adductor tubercle, and the bone is then slowly opened up to the point where the weightbearing goes through the center of the knee.Calculations of the specific amount of opening that is needed using the current digital x-ray systems are very accurate. Concurrent with this, a plate and screws are placed on the outside of the knee and bone graft is placed into the opening wedge which is created to assist with healing of the gap.
How to Recover from a Distal Femoral Osteotomy
Patients who have a distal femoral osteotomy, which is basically a surgical fracture, need to be on crutches until the osteotomy heals sufficiently to start weightbearing. Otherwise, there is a risk that the hinge on the inside part of the knee could crack or the screws could break because too much weight is being placed on them from relying on the plate and screws to hold the fracture apart rather than allowing the bone to heal. In general, we keep patients non-weightbearing for 8 weeks for the distal femoral osteotomy, obtain x-rays at 8 weeks to ensure there is sufficient healing, and then initiate a partial protective weightbearing program, advancing it one-quarter body weight per week until the 3-month point. Further x-rays are obtained at that point to verify healing.As part of the planning for a distal femoral osteotomy, we like to put most of our patients into a lateral compartment unloader brace. These braces help push the weight towards the inside of the knee, and by doing so, they can help serve as an excellent screen to determine if a patient would benefit from a distal femoral osteotomy. In our hands, almost all patients who benefit from the use of a lateral unloader brace do very well with a later performed distal femoral osteotomy and are able to correct the knock knee condition.
The success rate of distal femoral osteotomies is felt to be about 70% to 75% at 10 years. The success rate also depends upon the amount of arthritis of the lateral compartment, if there is a concurrent meniscal transplant or cartilage resurfacing procedure, and also if the patient is not significantly overweight (with a high body mass index, BMI). In general, patients who smoke are not candidates for a distal femoral osteotomy because bone does not heal very well in smokers and this would generally be a contraindicated surgical procedure in this circumstance.
When is a distal femoral osteotomy performed for ligament tears?
Distal femoral osteotomies are most commonly performed with chronic MCL tears or ACL tears. In patients who have chronic MCL tears that are symptomatic, the peer reviewed literature notes that the patients who are in valgus alignment have a much higher risk of having their future MCL reconstruction graft procedure stretch out unless the malalignment is corrected with a distal femoral osteotomy.We have found that performing the distal femoral osteotomy and the MCL reconstruction at the same time is successful and does not require two separate reconstructions. For patients with ACL deficiencies, if they have significant arthritis in their lateral compartment with valgus alignment, then a concurrent ACL reconstruction with a distal femoral osteotomy may be indicated. In addition, there are some patients who may have a cartilage replacement surgery and/or a lateral meniscal transplant with their ACL reconstructions.
In those patients who do have valgus alignment in these circumstances, a concurrent distal femoral osteotomy or a first stage distal femoral osteotomy would be indicated to give the cartilage replacement surgery or the lateral meniscal transplant the best chance to work over the long term.
When is a distal femoral osteotomy performed for osteoarthritis?
A distal femoral osteotomy can be performed for osteoarthritis when one has had development of osteoarthritis on the outside part of their knee, their knee alignment has become knock knee and is in valgus, and whereby the cartilage and the meniscus on the inside of the knee is still in good condition to whereby shifting the weight towards the inside of the knee would benefit the patient. In general, one should be between the ages of 16 (with closed growth plates) and a roughly upper age of 55 to benefit from a distal femoral osteotomy.The workup of this includes long leg x-rays to confirm that the patient is malaligned and does have valgus alignment, one has an arthroscopic surgery or an MRI to confirm that the cartilage on the inside part of the knee is fairly intact, as well as the majority of the medial meniscus and that one has intact ligaments or plan to reconstruct the ligaments either concurrently or thereafter the osteotomy. Oftentimes, we will place the patient into a lateral compartment unloader brace to use as a screen to determine that a distal femoral osteotomy may be a useful procedure. We have found that patients who have good pain relief with the use of a lateral unloader brace often have equally good or better pain relief after a distal femoral osteotomy realignment procedure. This is a good option for patients with knock knee.
What is the surgical technique for a distal femoral osteotomy?
There are two main surgical techniques for a distal femoral osteotomy. These are the lateral opening wedge osteotomy, whereby a bone wedge is placed into the outside portion of the femur to change the alignment or a closing wedge medial distal femoral osteotomy, whereby a bone wedge is taken out and the bone is collapsed down to change the alignment. In general, we mainly perform an opening wedge distal femoral osteotomy to realign the knee. Other than concurrently either adding bone or taking out bone, there may not be a big difference between either technique. The most important technique, therefore, would be the one that one’s surgeon feels most comfortable with performing a distal femoral osteotomy.When should one choose a distal femoral osteotomy or go directly to a total knee replacement?
In general, patients who wish to remain relatively high impact, especially laborers or patients who are still pretty active, or in younger patients, a distal femoral osteotomy would be preferred over a total knee replacement. There are often many symposia and debates at national and international meetings on this topic. In general, it is felt that younger patients definitively should have a distal femoral osteotomy when it is indicated, whereas older patients may equally benefit from a distal femoral osteotomy or a total knee replacement, depending upon their overall activity levels, if they have other medical problems, and if their bone is relatively osteopenic (softer than normal).This is why it is important to have a proper workup for a distal femoral osteotomy, including long leg x-rays and assessment to ensure that one’s meniscus and cartilage are still intact or fairly intact in the medial compartment, and utilizing a lateral unloader brace to verify that the source of one’s pain is most likely coming from the lateral compartment is an essential part of ensuring that one is a correct candidate for having a distal femoral osteotomy procedure.
What is the success rate of distal femoral osteotomies?
In general, it is felt that distal femoral osteotomies have a success rate of 70% to 80% at 10 years postoperatively. Most patients who did not have success during this timeframe were converted to a total knee replacement.When can one have painful hardware taken out after a distal femoral osteotomy?
In general, the plates and screws that are used to fix long bone fractures are left in for a minimum of one year prior to having them taken out. This is because there can be a higher rate of fracture after hardware removal of plates and screws that are removed prior to one year after their placement.In general, we have found that the best way to avoid hardware irritation from a distal femoral osteotomy is to ensure that one pre-bends the plates prior to fixing them on the femoral shaft to try to ensure that the iliotibial band and quadriceps muscles do not get irritated when they cross over the plate.
Unfortunately, pre-bending the plate may not always be successful at eliminating future hardware irritation in smaller patients, so these patients may have to wait until the osteotomy is completely healed and a minimum of one year after surgery prior to having the plate and screws that are causing any of the hardware irritation removed.