Tibial Tubercle Osteotomy
Femoral derotational osteotomy, commonly referred to as derotational osteotomy, is a surgical solution utilized to address issues related to knee instability, arthritis, or cartilage defects affecting the patellofemoral joint (the junction between the kneecap and the thigh bone). During this surgical procedure, a section of bone near the femur (thigh bone) is repositioned or rotated to correct the underlying problem.
Candidates for femoral derotational osteotomy typically include individuals who exhibit specific knee-related concerns such as:
- Patellar Instability: Those experiencing patellar instability caused by forces that displace the kneecap dislocation from its natural track, especially when a soft tissue procedure like medial patellofemoral ligament reconstruction may not be the most suitable option.
- Patellar Malalignment: Patients with pain attributed to misalignment of the patella, resulting in excessive strain and stress-related cartilage damage in the anterior region of the knee.
- Patellofemoral Arthritis: Individuals diagnosed with patellofemoral arthritis, also known as chondromalacia, softening of the cartilage, coupled with associated cartilage damage.
Common symptoms associated with these conditions include a specific kind of stiffness and pain in the front of the knee, often experienced after prolonged periods of sitting, such as during extended flights or at theatrical performances. Additionally, transitioning from a seated to standing position can trigger discomfort. Activities involving squats, lunges, stair climbing, especially descending, may exacerbate these symptoms. For women, wearing high-heeled footwear may also be painful due to the underlying knee issues addressed by femoral derotational osteotomy.
Tibial Tubercle Transfer at KNEECARES – The Superspeciality Knee Clinic
At our center, patients experiencing pain and/or instability in their joints undergo a comprehensive evaluation process, which encompasses a detailed physical examination and a thorough review of their medical history. As part of this evaluation, magnetic resonance imaging (MRI) is utilized to provide invaluable insights into the condition of the joint's cartilage, particularly in the patellofemoral joint. This diagnostic tool aids in determining whether the patient is an appropriate candidate for a specific surgical procedure called femoral derotational osteotomy.
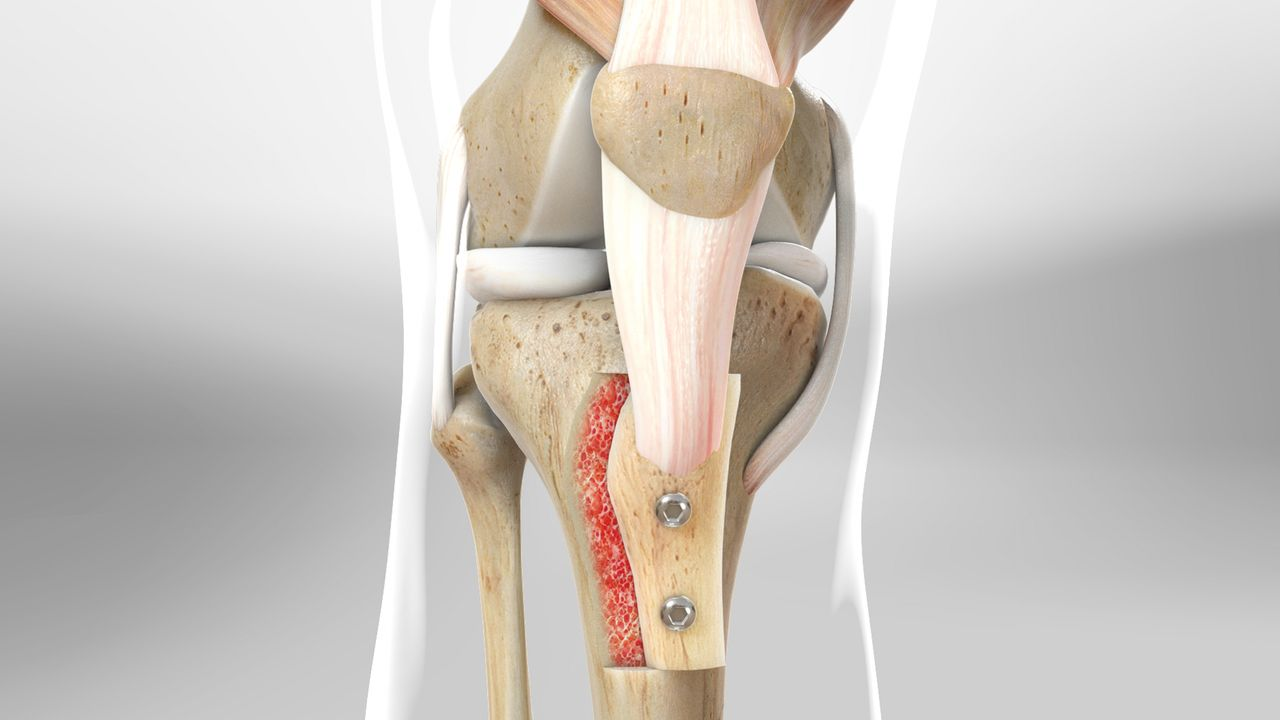
During the Femoral derotational osteotomy procedure, our surgical team takes meticulous care to ensure that the transferred bone aligns with the patellar tendon, allowing for precise guidance of the kneecap into the femoral groove, where the patellofemoral joint is located. Furthermore, we make every effort to alleviate pressure from any areas where cartilage damage has occurred.
To maintain the newly corrected bone position, two screws are skillfully inserted to secure it in place. It's important to note that, should these screws become bothersome to the patient at any point during their recovery, they can be removed through a subsequent procedure. This flexibility ensures that our patients receive the most suitable knee cares Treatment tailored to their individual needs and comfort.
Recovery from Tibial Tubercle Transfer
During the recovery period following femoral derotational osteotomy, it's of utmost importance to ensure proper bone healing before allowing the patient to bear any weight on the affected leg. For the initial six weeks post-surgery, patients are advised to rely on crutches for mobility assistance. In addition to this, a valuable tool in the recovery process is the utilization of a continuous passive motion machine (CPM) at home.
The CPM device plays a pivotal role in preventing joint stiffness and minimizing the formation of scar tissue by gently moving the knee without requiring any active muscle engagement. Throughout this early recovery phase, the affected leg is maintained in a brace, except during CPM usage. Adhering to these post-operative guidelines is vital to the overall success of the surgical procedure.
Assuming that the healing process progresses as anticipated and the quadriceps muscle attains adequate strength, the transition to physical therapy and weight-bearing exercises generally commences around the six-week mark. While individual recovery rates may vary, most patients find themselves able to return to work or school within approximately two weeks, gradually resume various forms of exercise between four and five months, and often regain the ability to engage in sports activities approximately nine months post-surgery.
Femoral derotational osteotomy is a procedure that boasts a track record of success when appropriately selected for patients, and it is typically well-tolerated and safe. However, as with any surgical intervention, there are potential rare complications to be aware of. These include the risk of blood clot formation, the possibility of infection, and the occurrence of fractures or delayed bone healing. To mitigate these risks, proactive measures are taken, such as discontinuing the use of birth control pills prior to surgery and abstaining from smoking for at least one month before the operation and throughout the entire duration of the recovery process. These precautions contribute to the overall safety and effectiveness of femoral derotational osteotomy for our patients.